Background/Purpose: In addition to traditional rheumatic diseases (TRDs), Pediatric Rheumatologists are often consulted on emerging rheumatic diseases (ERDs) such as autoimmune encephalitis, seronegative vasculitides, and immune dysregulation. There is little data on the presentation and outcomes for children with these conditions in the critical care setting. The objective of this study was to compare differences in presentation and outcomes for Rheumatology consultation for patients with both traditional and emerging rheumatic diseases admitted to the critical care setting at a quaternary care hospital.
Methods: A retrospective chart review for all consecutive consults in the critical care setting from March 2012-2016 was completed. We collected clinical data from admission, consult, and discharge, and scores from PCPC (Pediatric Cerebral Performance Category), and POPC (Pediatric Overall Performance Category). Summary statistics were stratified by diagnosis and compared using generalized estimating equations (GEE) to account for multiple admissions. GEE was used to estimate odds ratios for acquiring a cognitive disability while in the ICU.
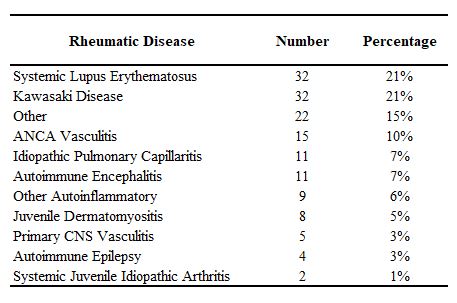
Results: There were 269 consecutive consultations (250 unique patients). 56.1% (151) required Rheumatology intervention; 70.9% (107) were classified as TRDs, 29% (44) were classified as ERDs. TRDs had more shock at admission (54.2% vs. 22.7%, p=0.001) and more organ dysfunction: cardiovascular (70.1% vs. 29.5%, p< 0.001), inotropes (37.4% vs. 4.5%, p=0.001), pericardial effusion (21.5% vs. 2.3%, p=0.018), pleural effusion (23.4% vs. 4.5%, p=0.014), renal (37.4% vs. 15.9%, p=0.012), liver/GI (57% vs. 29.5%, p=0.003), and more acquired a global functional disability while in the ICU (56.8% vs. 34.3%, p=0.028). ERDs had a longer median time to consult (2.5 days vs. 1 day, p=0.042), and longer median hospital LOS (15 days vs. 10 days, p=0.047). More CNS involvement (54.5% vs. 24.3%, p< 0.001), with altered mental status (52.3% vs. 15.9%, p< 0.001), and seizures (40.9% vs. 5.6%, p< 0.001). ERDs had more respiratory failure (77.3% vs. 42.1%, p< 0.001), intubation (41.2% vs. 17.8%, p=0.044), pulmonary hemorrhage (25% vs. 8.4%, p=0.009), mechanical ventilation the 1st hour (37.1% vs. 11.1%, p=0.002) and first 24 hours (45.7% vs. 16%, p=0.001). ERDs were more often discharged to inpatient rehabilitation (18.2% vs. 5.6%, p=0.048), and had mild cognitive disability at baseline (22.9% vs. 6.2%, p=0.013) and discharge (31.4% vs. 9.9%, p=0.014). After adjusting for baseline cognitive disability, ERDs had 6.4 times higher odds (95% CI: 1.84, 22.03) of acquiring a cognitive disability while in the ICU.
Conclusion: These data illustrate a phenotypic difference between TRDs who presented with more serositis, shock and multi-organ dysfunction, and ERDs who had more neurological involvement, pulmonary hemorrhage, mechanical ventilation, cognitive disability and rehabilitation needs. These data also show a delay in Rheumatology consultation for ERDs vs. TRDs. Continued education may be warranted regarding early identification of these emerging inflammatory conditions.
The post Pediatric Rheumatology Consultation for Both Traditional and Emerging Rheumatic Diseases in the Critical Care Setting appeared first on ACR Meeting Abstracts.